Overview
The digestive system is responsible for the breakdown and absorption of food and the elimination of waste. It consists of the gastrointestinal tract (a continuous tube from mouth to anus) and several accessory organs that assist in digestion. The system functions through five primary processes: motility moves food through the tract, secretion delivers enzymes and other digestive fluids, digestion breaks down food mechanically and chemically, absorption transfers nutrients into the bloodstream, and elimination expels undigested material.
| Function | Description |
|---|---|
| Motility | Ingestion, mastication, deglutition, peristalsis |
| Secretion | Enzymes, acid, bile, mucus |
| Digestion | Mechanical and chemical breakdown of food |
| Absorption | Nutrients, water, electrolytes |
| Elimination | Defecation |
The GI tract is organized into distinct segments, each specialized for particular aspects of digestion. The wall of the tract shares a common structural plan throughout its length, with regional variations that reflect local function.
General Histology of GI Tract
The wall of the gastrointestinal tract is composed of four concentric layers. From inner to outer, these are the mucosa, submucosa, muscularis externa, and serosa (or adventitia). This layered organization is consistent from the esophagus through the rectum, though the specific features of each layer vary by region.
Four Layers
| Layer | Subdivisions | Function |
|---|---|---|
| Mucosa | Epithelium, lamina propria, muscularis mucosae | Absorption, secretion, protection |
| Submucosa | Connective tissue, vessels, nerves (Meissner plexus) | Support, blood supply |
| Muscularis externa | Inner circular, outer longitudinal (myenteric plexus between) | Peristalsis, segmentation |
| Serosa (intraperitoneal) or Adventitia (retroperitoneal) | Connective tissue + mesothelium (serosa) | Outer covering |
The mucosa is the innermost layer and is responsible for most digestive and absorptive functions. Its epithelium varies regionally: stratified squamous in areas subject to mechanical abrasion (mouth, esophagus), and simple columnar where secretion and absorption occur (stomach, intestines). The lamina propria is a layer of loose connective tissue containing blood vessels, lymphatics, and immune cells. The muscularis mucosae, a thin layer of smooth muscle, causes local movement of the mucosa.
The submucosa provides mechanical support and contains the submucosal plexus (Meissner plexus), which innervates the mucosa and regulates secretion and blood flow. The muscularis externa generates the propulsive forces of digestion. Its inner circular fibers constrict the lumen, while outer longitudinal fibers shorten the tract. Between these muscle layers lies the myenteric plexus (Auerbach plexus), which controls motility.
Enteric Nervous System
The enteric nervous system is the intrinsic nervous system of the GI tract, often called the “second brain.” It can function independently of the central nervous system, though it receives modulation from autonomic inputs.
| Plexus | Location | Function |
|---|---|---|
| Myenteric (Auerbach) | Between circular and longitudinal muscle | Motility |
| Submucosal (Meissner) | Within submucosa | Secretion, absorption, blood flow |
Oral Cavity
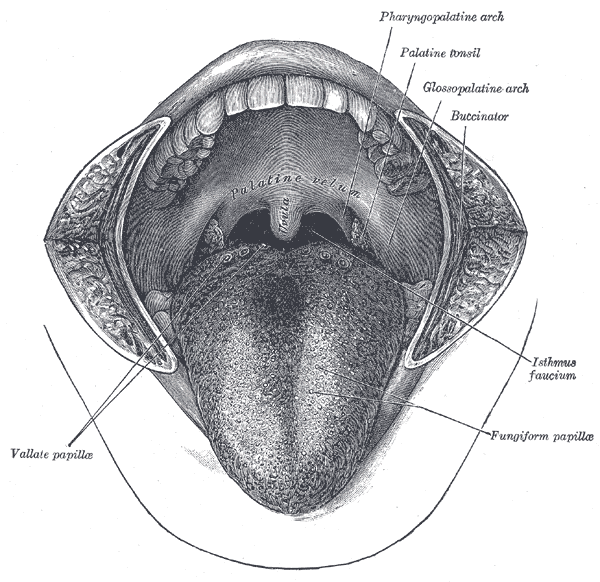
The oral cavity is the entry point of the digestive system, where food is ingested, mechanically broken down by mastication, and mixed with saliva to begin chemical digestion. The mouth is bounded by the lips anteriorly, the cheeks laterally, the palate superiorly, and the tongue inferiorly.
| Structure | Description |
|---|---|
| Lips (labia) | Orbicularis oris muscle, vermilion border |
| Cheeks (buccae) | Buccinator muscle |
| Palate (hard/soft) | Hard: Maxilla + palatine bones; Soft: Muscular (uvula) |
| Tongue | Intrinsic (shape, CN XII) + extrinsic (genioglossus, hyoglossus, styloglossus, palatoglossus) muscles |
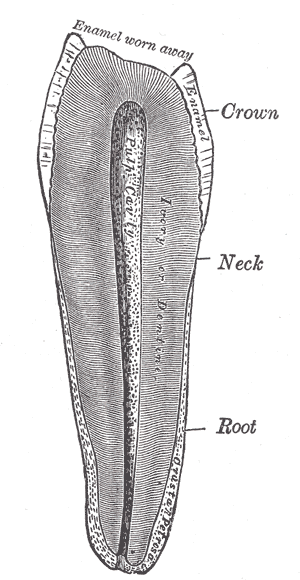
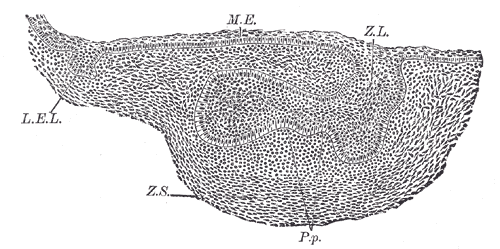
| Teeth | 20 deciduous, 32 permanent (8 incisors, 4 canines, 8 premolars, 12 molars) |
| Salivary glands | Parotid (CN IX), submandibular (CN VII), sublingual (CN VII), minor glands |
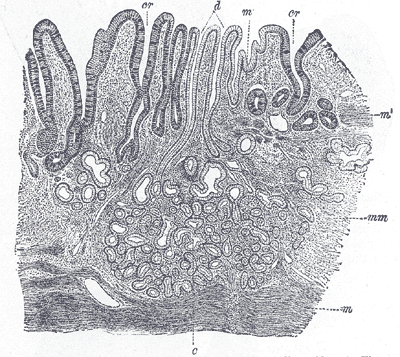
The tongue is a muscular organ essential for mastication, swallowing, and speech. Intrinsic muscles alter the tongue’s shape, while extrinsic muscles control its position. The dorsal surface is covered by papillae (filiform, fungiform, circumvallate, foliate), which contain taste buds. The tongue’s rich blood supply comes from the lingual artery, a branch of the external carotid.
Saliva is produced by three pairs of major salivary glands (parotid, submandibular, sublingual) and numerous minor glands. Saliva contains amylase (begins starch digestion), lipase, mucus, immunoglobulins (IgA), and antibacterial enzymes (lysozyme). The parotid gland secretes primarily serous fluid via the parotid duct (Stensen duct), opening at the buccal mucosa opposite the second maxillary molar.
Pharynx and Esophagus
The pharynx is the common passageway for food and air, connecting the oral cavity to the esophagus. Deglutition (swallowing) occurs in three phases: the oral phase (voluntary), the pharyngeal phase (involuntary, reflexive), and the esophageal phase (involuntary, peristaltic).
The esophagus is a muscular tube approximately 25 cm long that transports food from the pharynx to the stomach. It passes through the superior and posterior mediastinum and enters the abdomen through the esophageal hiatus of the diaphragm at T10.
| Feature | Description |
|---|---|
| Length | 25 cm (from pharynx to stomach) |
| Sphincters | Upper (UES, cricopharyngeus), Lower (LES, gastroesophageal) |
| Constrictions | Cervical (UES), aortic arch, left main bronchus, diaphragmatic |
| Epithelium | Stratified squamous (non-keratinized) |
| Musculature | Upper 1/3 skeletal, middle mixed, lower 1/3 smooth |
| Blood supply | Thyroid (cervical), bronchial/aortic (thoracic), left gastric/phrenic (abdominal) |
| Innervation | Vagus (parasympathetic), sympathetic trunk |
The lower esophageal sphincter (LES) is a physiological sphincter maintained by the tonic contraction of smooth muscle and the pinch of the diaphragmatic crura. It prevents reflux of gastric contents. Incompetence of the LES leads to gastroesophageal reflux disease (GERD).
Stomach
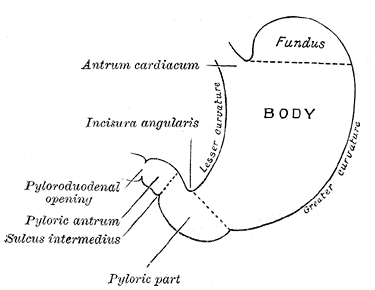
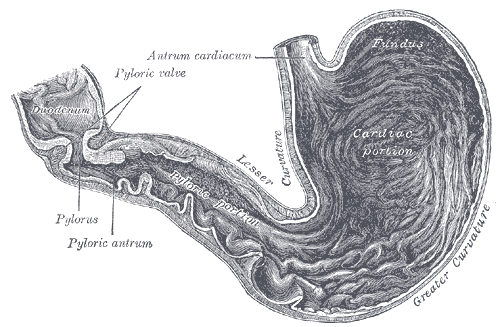
The stomach is a J-shaped organ that serves as a reservoir for food and the site of mechanical and chemical digestion. It receives the bolus from the esophagus, mixes it with gastric secretions to form chyme, and regulates its release into the duodenum. The stomach has a capacity of approximately 1-1.5 liters in adults and can expand significantly during a meal.
| Feature | Description |
|---|---|
| Capacity | ~1-1.5 L (adult) |
| Regions | Cardia, fundus, body, antrum, pylorus |
| Curvatures | Lesser (lesser omentum), greater (greater omentum) |
| Sphincters | Lower esophageal (cardiac), pyloric |
| Epithelium | Simple columnar (mucus, parietal, chief, G cells, enterochromaffin) |
| Mucosal folds | Rugae (allow distension) |
| Blood supply | Celiac trunk (left gastric, splenic, common hepatic → right gastric, gastroepiploic) |
| Innervation | Vagus (anterior/posterior trunks), celiac plexus |
The gastric mucosa is lined by a simple columnar epithelium that invaginates to form gastric pits and glands. The type of gland varies by region: cardiac glands (predominantly mucus-secreting) in the cardia, gastric glands (containing parietal and chief cells) in the fundus and body, and pyloric glands (containing G cells) in the antrum.
Gastric Gland Cells
| Cell | Secretion | Function |
|---|---|---|
| Parietal (oxyntic) | HCl, intrinsic factor | Acid (pH 1-3), B₁₂ absorption |
| Chief (peptic) | Pepsinogen | Protein digestion (activated to pepsin) |
| Mucous neck cell | Mucus | Protection |
| G cell (antrum) | Gastrin | Stimulates acid secretion |
| D cell | Somatostatin | Inhibits acid secretion |
| Enterochromaffin-like (ECL) | Histamine | Stimulates acid secretion |
Parietal cells secrete hydrochloric acid through an H⁺/K⁺ ATPase pump, creating a luminal pH of 1-3. This acidic environment activates pepsinogen to pepsin, kills ingested microorganisms, and facilitates mineral absorption. Parietal cells also secrete intrinsic factor, a glycoprotein essential for vitamin B₁₂ absorption in the ileum. Loss of parietal cells (as in autoimmune gastritis) leads to pernicious anemia.
Small Intestine
The small intestine is the primary site of nutrient absorption, measuring approximately 6 meters in length. It is divided into three segments: duodenum, jejunum, and ileum. The small intestine’s absorptive surface area is vastly increased by three structural features: the plicae circulares (circular folds), villi (finger-like projections), and microvilli (brush border).
| Section | Length | Function |
|---|---|---|
| Duodenum | 25 cm | Mixing with bile/pancreatic enzymes, iron/calcium absorption |
| Jejunum | 2.5 m | Most nutrient absorption (carbohydrates, proteins, fats) |
| Ileum | 3.5 m | Bile salts, vitamin B₁₂ absorption |
Duodenum
The duodenum is the shortest segment and receives chyme from the stomach. It is retroperitoneal except for its first part. The common bile duct and main pancreatic duct join at the hepatopancreatic ampulla (of Vater), which opens into the descending duodenum at the major duodenal papilla. The sphincter of Oddi regulates bile and pancreatic juice flow.
| Part | Level | Description | Relations |
|---|---|---|---|
| Superior (1st) | L1 | Duodenal bulb | Gallbladder, liver |
| Descending (2nd) | L1-L3 | Contains major papilla | Head of pancreas, common bile duct + pancreatic duct |
| Horizontal (3rd) | L3 | Crossed by SMA/SMV | Superior mesenteric vessels |
| Ascending (4th) | L3→L2 | Duodenojejunal flexure | Ligament of Treitz |
Villi and Microvilli
The plicae circulares are permanent circular folds of mucosa and submucosa that are most prominent in the jejunum. Villi are 0.5-1.5 mm finger-like projections of mucosa that contain a central lymphatic capillary (lacteal) and a capillary network. Each epithelial cell bears microvilli (the brush border), which contain digestive enzymes and transporter proteins.
Absorption by Nutrient
| Nutrient | Site | Mechanism |
|---|---|---|
| Carbohydrates | Jejunum | Monosaccharide transporters (SGLT1, GLUT2, GLUT5) |
| Proteins | Jejunum | Amino acid transporters, di/tripeptide transporters (PepT1) |
| Fats | Jejunum | Micelles → chylomicrons (via lymph) |
| Iron | Duodenum | DMT1 (heme), ferroportin (export) |
| Calcium | Duodenum | TRPV6 (vitamin D-dependent) |
| Bile salts | Ileum | Active transport (enterohepatic circulation) |
| Vitamin B₁₂ | Ileum | Intrinsic factor-dependent |
Large Intestine
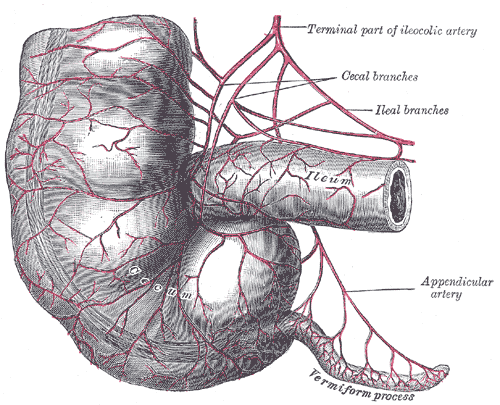
The large intestine absorbs water and electrolytes, forms and stores feces, and houses the gut microbiome. It is approximately 1.5 meters long and consists of the cecum, appendix, colon (ascending, transverse, descending, sigmoid), rectum, and anal canal.
| Section | Length | Function |
|---|---|---|
| Cecum | 6-8 cm | Ileocecal valve, appendix |
| Appendix | 8-10 cm | Immune (lymphoid tissue) |
| Colon (ascending, transverse, descending, sigmoid) | 1.5 m | Water/electrolyte absorption, feces formation |
| Rectum | 12-15 cm | Storage |
| Anal canal | 3-4 cm | Defecation (internal/external sphincters) |
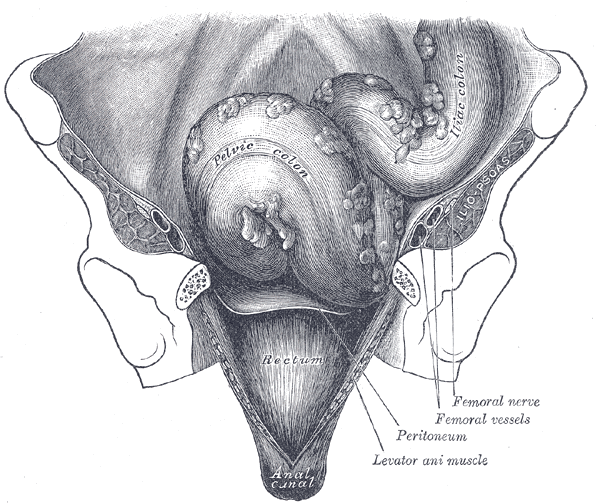
The large intestine is distinguished from the small intestine by several features. The taeniae coli are three longitudinal bands of smooth muscle that run the length of the colon. Their tonic contraction produces haustra, the sacculations that give the colon its characteristic appearance. Appendices epiploicae are small pouches of peritoneum filled with fat that hang from the colonic surface.
The epithelium of the large intestine is simple columnar with abundant goblet cells that secrete mucus for lubrication. Unlike the small intestine, there are no villi. The mucosa contains numerous intestinal glands (crypts of Lieberkühn) lined with absorptive cells and goblet cells.
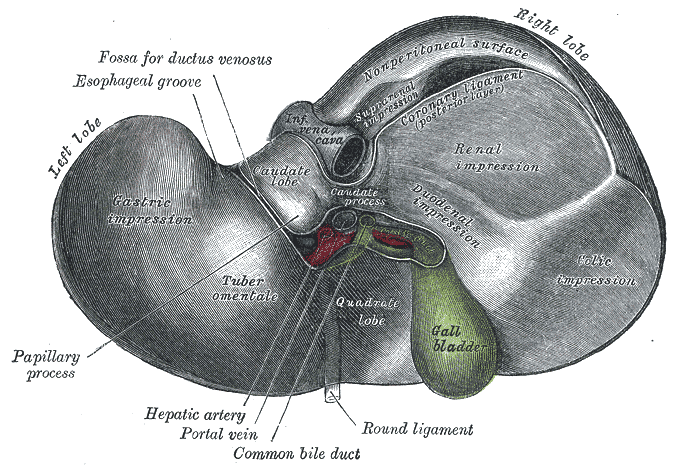
Liver
The liver is the largest internal organ (1400-1600 g), located in the right upper quadrant. It performs over 500 functions, including metabolism, detoxification, protein synthesis, bile production, and glycogen storage.
| Feature | Description |
|---|---|
| Weight | 1400-1600 g |
| Location | Right upper quadrant (RUQ) |
| Lobes | Right (largest), left, caudate, quadrate |
| Ligaments | Falciform, round (ligamentum teres), coronary, triangular |
Microscopic Structure
The liver is organized into structural and functional units called lobules. The classic lobule is hexagonal with a central vein at its center and portal triads at its periphery. Each portal triad contains a branch of the hepatic artery, a branch of the portal vein, and a bile ductule.
| Unit | Structure |
|---|---|
| Classic lobule | Central vein → hepatocyte plates → portal triads |
| Portal lobule | Bile duct centered |
| Acinus | Zone 1 (periportal), Zone 2 (midzonal), Zone 3 (perivenular) |
Blood flows from the portal triad toward the central vein through sinusoids lined by fenestrated endothelium. Hepatocytes are arranged in plates one or two cells thick, with bile canaliculi between them. Kupffer cells are hepatic macrophages lining the sinusoids that phagocytose pathogens and debris. Stellate (Ito) cells in the space of Disse store vitamin A and, when activated, produce the collagen that characterizes cirrhosis.
Biliary System
| Structure | Description |
|---|---|
| Bile canaliculi | Between hepatocytes → bile ducts |
| Right and left hepatic ducts | Merge to common hepatic duct |
| Common hepatic duct + cystic duct | → Common bile duct |
| Common bile duct + pancreatic duct | → Hepatopancreatic ampulla (Sphincter of Oddi) |
| Gallbladder | 30-50 mL, stores/concentrates bile |
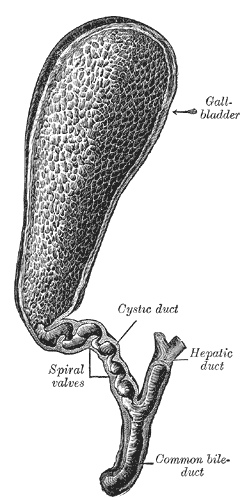
Bile is produced by hepatocytes and flows through the canaliculi into bile ducts. The gallbladder stores and concentrates bile between meals. Upon stimulation by cholecystokinin (CCK), the gallbladder contracts and releases bile into the common bile duct. Bile emulsifies fats, facilitates absorption of fat-soluble vitamins (A, D, E, K), and eliminates bilirubin and cholesterol.
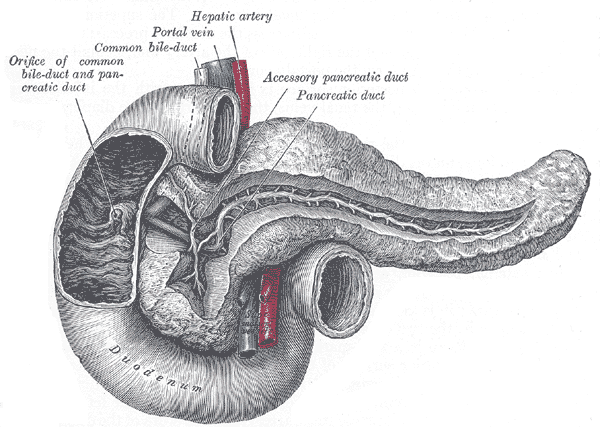
Pancreas
The pancreas is a retroperitoneal organ weighing 80-100 g that has both exocrine and endocrine functions. It lies transversely in the epigastrium, with its head nestled in the C-curve of the duodenum.
| Feature | Description |
|---|---|
| Weight | 80-100 g |
| Location | Retroperitoneal (epigastrium) |
| Parts | Head (uncinate process), neck, body, tail |
| Duct | Main pancreatic (Wirsung), accessory (Santorini) |
Exocrine Pancreas
The exocrine pancreas consists of acinar cells arranged in clusters (acini) that secrete digestive enzymes into a ductal system. The ductal cells secrete bicarbonate-rich fluid that neutralizes gastric acid in the duodenum, creating an optimal pH for pancreatic enzyme activity.
| Cell type | Secretion | Function |
|---|---|---|
| Acinar cells | Digestive enzymes (trypsinogen, chymotrypsinogen, amylase, lipase, nucleases) | Digestion |
| Ductal cells | Bicarbonate-rich fluid | Neutralizes gastric acid |
Endocrine Pancreas (Islets of Langerhans)
Scattered throughout the exocrine pancreas are the islets of Langerhans, endocrine cell clusters that secrete hormones regulating blood glucose metabolism. The islets are richly vascularized and receive autonomic innervation.
| Cell | Hormone | Function |
|---|---|---|
| Beta (β) | Insulin | ↓ Blood glucose |
| Alpha (α) | Glucagon | ↑ Blood glucose |
| Delta (δ) | Somatostatin | Paracrine inhibition |
| PP (γ) | Pancreatic polypeptide | GI regulation |
| Epsilon (ε) | Ghrelin | Appetite stimulation |
Blood Supply
The arterial supply of the digestive system is organized by embryonic origin: the foregut (stomach, duodenum, liver, pancreas, spleen) is supplied by the celiac trunk; the midgut (jejunum through proximal transverse colon) by the superior mesenteric artery; and the hindgut (distal transverse colon through rectum) by the inferior mesenteric artery.
| Artery | Territory |
|---|---|
| Celiac trunk | Foregut (stomach, duodenum, liver, pancreas, spleen) |
| Superior mesenteric (SMA) | Midgut (jejunum, ileum, cecum, appendix, ascending colon, proximal 2/3 transverse colon) |
| Inferior mesenteric (IMA) | Hindgut (distal 1/3 transverse colon, descending colon, sigmoid colon, rectum) |
Venous (Portal System)
The portal venous system collects nutrient-rich blood from the GI tract and delivers it to the liver for processing. The portal vein is formed by the union of the superior mesenteric vein (draining the midgut) and the splenic vein (draining the foregut). The inferior mesenteric vein drains the hindgut and typically joins the splenic vein. Portal vein blood flows through the liver sinusoids (where hepatocytes process absorbed nutrients and remove toxins) and exits via the hepatic veins into the inferior vena cava.
Innervation
The GI tract receives both extrinsic autonomic innervation (parasympathetic and sympathetic) and possesses an extensive intrinsic nervous system (enteric nervous system). The parasympathetic input (primarily via the vagus nerve) promotes digestion by increasing motility, secretion, and blood flow. Sympathetic input (via the splanchnic nerves) inhibits digestion during stress or exercise.
| Nerve | Function |
|---|---|
| Vagus (parasympathetic) | Increases motility, secretion, relaxation of sphincters |
| Splanchnic (sympathetic) | Decreases motility, secretion, vasoconstriction, sphincter contraction |
| Enteric (intrinsic) | Local reflexes (peristalsis, secretion) |